
User:Tdamm1992/sandbox
Classification
Kidney masses can be classified by the nature of the cells in the growth, or by its appearance on radiography. [1] The term cancer refers to a malignant tumor, which is an uncontrolled growth of abnormal cells.[2] However, kidney masses can be due to growth of normal tissue (benign), inflammatory (a reaction of the immune system), or vascular (cells of the blood vessels). Radiologically tumors are grouped based on appearance into simple cystic, complex cystic, or solid.[1]
The most common type of kidney malignancy is renal cell carcinoma[3] which is thought to originate from cells in the proximal convoluted tubule. [4] [5] Another type of kidney cancer although less common, is transitional cell cancer (TCC) or urothelial carcinoma of the renal pelvis. [6]The renal pelvis is the part of the kidney that collects urine and drains it into a tube called the ureter. [6] The cells that line the renal pelvis are called transitional cells, and are also sometimes called urothelial cells. The transitional/urothelial cells in the renal pelvis are the same type of cells that line the ureter and bladder. For this reason TCC of the renal pelvis is distinct from RCC and behaves more like bladder cancer. [6] Other types of kidney cancers that can arise from the urothelial cells of the renal pelvis are squamous cell carcinoma and adenocarcinoma,[4] similar to those that arise from bladder urothelial cells.
Other causes of kidney cancer include the following:
- Sarcoma
- Metastatic tumor from distant organ
- Lymphoma
- Wilms tumor- an embryonic tumor that is the most common type of kidney cancer in children
Renal cell carcinoma can be further classified based on histological appearance.
- Juxtaglomerular cell tumor (reninoma)
- Angiomyolipoma
- Bellini duct carcinoma
- Clear-cell sarcoma of the kidney
- Mesoblastic nephroma
- Mixed epithelial stromal tumor[7]
Rarely, some other types of cancer and potentially cancerous tumors that more usually originate elsewhere can originate in the kidneys. These include:
- Clear cell adenocarcinoma
- Inverted papilloma
- Teratoma[8]
- Carcinosarcoma[9]
- Carcinoid tumor of the renal pelvis[10]
Cancer in the kidney may also be secondary, the result of metastasis from a primary cancer elsewhere in the body.
Signs and symptoms[edit]
Due to the anatomic location of the kidney, many renal masses do not cause any symptoms and are undetectable on physical examination until they are in a locally advanced stage.[11]
Historically kidney cancer presented with a triad of symptoms of hematuria, flank pain, and palpable mass on examination. This rarely occurs as the presenting symptoms today and may be a sign of locally advanced disease if it does occur. [11] Due to the increase in US and CT abdominal imaging for nonspecific abdominal complaints, the frequency of incidental kidney mass diagnosis on medical imaging has increased. [11][12][13] More than 60% of renal cell carcinoma (RCC: the most common type of kidney cancer), are diagnosed incidentally by abdominal imaging for nonspecific abdominal complaints. [11][14]
Other symptoms that are consistent of advanced disease include weight loss, fever, night sweats, palpable swollen lymph nodes in the cervical region, non-reducing varicocele, and bilateral lower leg swelling. These symptoms are consistent with systemic disease. [11]
Diagnosis and Evaluation[edit]
Radiographic Imaging[edit]
Since a suspected renal mass has a large differential diagnosis, the first step is to characterize the mass with radiographic imaging to assess the likelihood of a benign or malignant mass. Ultrasonography is sometimes used to evaluate a suspected kidney mass, as it can characterize cystic and solid kidney masses without radiation exposure and at relative low cost.[11] Simple cysts, which are defined by strict criteria[15] are safe to be monitored if the person does not have any symptoms.[11] However, all masses that are not clearly simple cysts should be further evaluated and confirmed by alternate imaging techniques.[16][11]
Computed Tomography (CT) of the abdomen administered with and without IV contrast is the ideal imaging to diagnose and stage kidney cancer. [13][16][11] Iodinated contrast agents can cause transient or permanent worsening of kidney function in patients with chronic kidney disease (CKD) with a glomerular filtration rate (GFR) less than 45ml/min/1.73m2 and should therefore be administered cautiously in these patients. [17]
Abdominal MRI is an alternative imaging method that can be used to characterize and stage a kidney mass [18][13][16][11] and may be suggested if contrast material cannot be administered [13]. MRI can also evaluate the inferior vena cava if the mass is suspected to extend outside the kidney.[13]
Since the lungs are the most common organ for kidney cancer to spread to, a chest X-ray or CT scan may be ordered based on the person’s risk for metastatic disease. [11][16]
Laboratory Studies[edit]
People with suspected kidney cancer should also have their kidney function evaluated to help determine treatment options. Blood tests to determine kidney function include a comprehensive metabolic panel (CMP), a complete blood count (CBC).[13][16] In addition, these tests help understand the overall health of the person, which can be affected by metastatic disease (disease that is outside of the kidney). For example, liver or bone involvement could result in abnormal liver enzymes, electrolyte abnormalities, or anemia. A urine sample should also be collected for urinalysis. [16][13]
Renal Mass Biopsy[edit]
The utility of RMB lies in that it can confirm malignancy with reliability, can direct therapy based on diagnosis, and can provide drainage.[16]
Once imaging has been completed, renal mass biopsy should be considered if there is a high likelihood that the mass is hematologic, metastatic, inflammatory or infectious.[16] These types of lesions would not be managed surgically, differing from cancer originating from the kidney. Cancer originating outside the kidney and lymphoma are managed systemically. [11][16]
RMB can accurately diagnose malignancy, however, it cannot reliably diagnose benign disease. In other words, if the biopsy shows cancer, there is a 99.8% chance that kidney cancer is present (Positive Predictive Value= 99.8%). A negative biopsy does not rule out a diagnosis of cancer. [19]
Staging[edit]
Renal cell carcinoma is the only type of kidney cancer that follows the TNM staging system defined within the American Joint Committee on Cancer 2010 revision (AJCC 2010). (wieder, walsh, ajcc).The TNM stagingsystem classifies the tumor, nodes and metastasis of the disease, and is widely used among cancer in other organs. that is currently used to stage kidney cancer is the American Joint Committee on Cancer 2010 revision (AJCC 2010). This system of staging only applies to renal cell carcinoma, and not other types of kidney tumors (wieder).
The following is a description of the AJCC 2010 TNM system
The primary tumor of renal cell carcinoma is described in the following table, as according to the AJCC 2010 7th Edition Cancer Staging Manual:
| Tx | Tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| T1 | Tumor ≤7cm; limited to kidney |
| T1a | Tumor ≤4cm; limited to kidney |
| T1b | Tumor 4-≤7cm; limited to kidney |
| T2 | Tumor >7cm; limited to kidney |
| T2a | Tumor 7-≤10cm; limited to kidney |
| T2b | Tumor >10cm; limited to kidney |
| T3 | Tumor extends to major veins or perinephric tissue but not into ipsilateral adrenal gland nor beyond Gerota's fascia |
| T3a | Tumor grossly extends into renal vein or its' segmental branches, or tumor invades perirenal and/or renal sinus fat but not beyond Gerota's fascia |
| T3b | Tumor grossly extends into vena cava below the diaphragm |
| T3c | Tumor grossly extends into vena cava above the diaphragm or invades the wall of the vena cava |
| T4 | Tumor invvades beyond Gerota's fascia |
Within the TNM staging system used to describe renal cell carcinoma, N is described where N1 describes regional lymph node metastasis and N0 denotes none. Similarly, M1 describes distant metastasis, while M0 describes no distant metastasis. [20] Once the cancer is described by the TNM staging system, the anatomic stage can be determined as shown by the table below. The stage has prognostic implications for the renal cell carcinoma. Renal Cell Carcinoma that is deemed metastatic is by definition Stage IV kidney cancer. The lungs are the most common site for metastasis ,[16] with other common sites including bone, brain, liver, adrenal gland and distant lymph nodes. [13][21]
| Tumor (T) | Lymph Node (N) | Metastasis (M) | |
| Stage I | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T1 or T2
T3 |
N1
N0 or N1 |
M0
M0 |
| Stage IV | T4
Any T |
Any N
Any N |
M0
M1 |
-
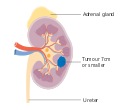 Stage 1 kidney cancer
Stage 1 kidney cancer -
 Stage 2 kidney cancer
Stage 2 kidney cancer -
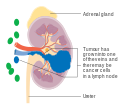 Stage 3 kidney cancer
Stage 3 kidney cancer -
 Stage 4 kidney cancer
Stage 4 kidney cancer




 | This is a user sandbox of Tdamm1992. You can use it for testing or practicing edits. This is not the sandbox where you should draft your assigned article for a dashboard.wikiedu.org course. To find the right sandbox for your assignment, visit your Dashboard course page and follow the Sandbox Draft link for your assigned article in the My Articles section. |
- ^ a b Campbell MD, Ph.D, Steven C.; Lane MD, Ph.D, Brian R. (2012). "Malignant Renal Tumors". In Wein MD, Ph.D, Alan J.; Kavoussi MD, MBA, Louis R. (eds.). Campbell-Walsh Urology. Elselvier. ISBN 978-1455775675.
- ^ "Cancer | Definition of Cancer by Lexico". Lexico Dictionaries | English. Retrieved 2019-11-12.
- ^ "Kidney Cancer | CDC". www.cdc.gov. 2019-07-09. Retrieved 2019-11-12.
- ^ a b Campbell MD, Ph.D, Steven C.; Lane MD, Ph.D, Brian R. (2012). "Malignant Renal Tumors". In Wein MD, Ph.D, Alan J.; Kavoussi MD, MBA, Louis R. (eds.). Campbell-Walsh Urology. Elselvier. ISBN 978-1455775675.
- ^ "Renal Cell Cancer Treatment (PDQ®)–Patient Version". National Cancer Institute. 2004-02-20. Retrieved 2019-11-12.
- ^ a b c "Transitional Cell Cancer of the Renal Pelvis and Ureter Treatment (PDQ®)–Patient Version". National Cancer Institute. 2004-02-20. Retrieved 2019-11-12.
- ^ Thyavihally YB, Tongaonkar HB, Desai SB (September 2005). "Benign mixed epithelial stromal tumor of the renal pelvis with exophytic growth: case report". Int Semin Surg Oncol. 2: 18. doi:10.1186/1477-7800-2-18. PMC 1215508. PMID 16150156.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ Nzegwu MA, Aligbe JU, Akintomide GS, Akhigbe AO (May 2007). "Mature cystic renal teratoma in a 25-year-old woman with ipsilateral hydronephrosis, urinary tract infection and spontaneous abortion". Eur J Cancer Care (Engl). 16 (3): 300–2. doi:10.1111/j.1365-2354.2006.00755.x. PMID 17508953.
- ^ Chiu, KC; Lin, MC; Liang, YC; Chen, CY (2008). "Renal carcinosarcoma: case report and review of literature". Renal Failure. 30 (10): 1034–9. doi:10.1080/08860220802403192. PMID 19016157.
- ^ Kuroda N, Katto K, Tamura M, Shiotsu T, Hes O, Michal M, Nagashima Y, Ohara M, Hirouchi T, Mizuno K, Hayashi Y, Lee GH (January 2008). "Carcinoid tumor of the renal pelvis: consideration on the histogenesis". Pathol. Int. 58 (1): 51–4. doi:10.1111/j.1440-1827.2007.02188.x. PMID 18067641.
- ^ a b c d e f g h i j k l Campbell MD, Ph.D, Steven C.; Lane MD, Ph.D, Brian R. (2012). "Malignant Renal Tumors". In Wein MD, Ph.D, Alan J.; Kavoussi MD, MBA, Louis R. (eds.). Campbell-Walsh Urology. Elselvier. ISBN 978-1455775675.
- ^ Sánchez-Martín, F. M.; Millán-Rodríguez, F.; Urdaneta-Pignalosa, G.; Rubio-Briones, J.; Villavicencio-Mavrich, H. (2008). "Small Renal Masses: Incidental Diagnosis, Clinical Symptoms, and Prognostic Factors". Advances in Urology. 2008. doi:10.1155/2008/310694. ISSN 1687-6369. PMC 2629071. PMID 19165347.
{{cite journal}}: CS1 maint: unflagged free DOI (link) - ^ a b c d e f g h Motzer, Robert J.; Jonasch, Eric; Agarwal, Neeraj; Bhayani, Sam; Bro, William P.; Chang, Sam S.; Choueiri, Toni K.; Costello, Brian A.; Derweesh, Ithaar H.; Fishman, Mayer; Gallagher, Thomas H. (2017-06-01). "Kidney Cancer, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology". Journal of the National Comprehensive Cancer Network. 15 (6): 804–834. doi:10.6004/jnccn.2017.0100. ISSN 1540-1405.
- ^ Silverman, Stuart G.; Israel, Gary M.; Herts, Brian R.; Richie, Jerome P. (2008-10). "Management of the incidental renal mass". Radiology. 249 (1): 16–31. doi:10.1148/radiol.2491070783. ISSN 1527-1315. PMID 18796665.
{{cite journal}}: Check date values in:|date=(help) - ^ Silverman, Stuart G.; Pedrosa, Ivan; Ellis, James H.; Hindman, Nicole M.; Schieda, Nicola; Smith, Andrew D.; Remer, Erick M.; Shinagare, Atul B.; Curci, Nicole E.; Raman, Steven S.; Wells, Shane A. (2019-06-18). "Bosniak Classification of Cystic Renal Masses, Version 2019: An Update Proposal and Needs Assessment". Radiology. 292 (2): 475–488. doi:10.1148/radiol.2019182646. ISSN 0033-8419.
- ^ a b c d e f g h i j "Renal Cancer: Renal Mass & Localized Renal Cancer Guideline - American Urological Association". www.auanet.org. Retrieved 2019-10-29.
- ^ Subramaniam, Rathan M.; Wilson, Renee F.; Turban, Sharon; Suarez-Cuervo, Catalina; Zhang, Allen; Sherrod, Cheryl; Aboagye, Jonathan; Eng, John; Choi, Michael J. (2016). Contrast-Induced Nephropathy: Comparative Effectiveness of Preventive Measures. AHRQ Comparative Effectiveness Reviews. Rockville (MD): Agency for Healthcare Research and Quality (US). PMID 26866209.
- ^ Janus, C. L.; Mendelson, D. S. (1991). "Comparison of MRI and CT for study of renal and perirenal masses". Critical Reviews in Diagnostic Imaging. 32 (2): 69–118. ISSN 1040-8371. PMID 1863349.
- ^ Patel, Hiten D.; Johnson, Michael H.; Pierorazio, Phillip M.; Sozio, Stephen M.; Sharma, Ritu; Iyoha, Emmanuel; Bass, Eric B.; Allaf, Mohamad E. (2016-5). "Diagnostic Accuracy and Risks of Biopsy in the Diagnosis of a Renal Mass Suspicious for Localized Renal Cell Carcinoma: Systematic Review of the Literature". The Journal of Urology. 195 (5): 1340–1347. doi:10.1016/j.juro.2015.11.029. ISSN 1527-3792. PMC 5609078. PMID 26901507.
{{cite journal}}: Check date values in:|date=(help) - ^ AJCC cancer staging manual. Edge, Stephen B., American Joint Committee on Cancer. (7th ed. ed.). New York: Springer. 2010. ISBN 9780387884400. OCLC 316431417.
{{cite book}}:|edition=has extra text (help)CS1 maint: others (link) - ^ "Kidney Cancer (Adult) – Renal Cell Carcinoma" (PDF). American Cancer Society. Archived from the original (PDF) on 2017-02-22. Last Revised: May 16, 2016